

Dr. Trask recommends...

Table of Contents
Coronavirus Inflicts its Own Kind of Terror
by M. T. Osterholm and M. Olshaker, The New York Times | Opinion
Coronavirus Inflicts its Own Kind of Terror
by Orhan Pamuk, The New York Times | Opinion
Not Like the Flu, Not Like Car Crashes, Not Like...
by A. Schulman, B. Foht & S. Matlack, The New Atlantis
Why Doesn't Flu Tank Economy Like Covid-19?
by Jo Craven McGinty, The Wall Street Journal
Covid-19: What's Wrong with the Models?
by Peter Attia, MD
Is the Virus on My Clothes? My Hair? My Shoes? My Newspaper?
by Tara Parker-Pope, The New York Times
10 Weeks to Crush the Curve
by Harvey V. Fineberg, The New England Journal of Medicine
COVID-19: Melatonin as a potential adjuvant treatment
by Rui Zhang, et al., Life Sciences
The Road Back to Normal
by Scott Gottlieb and Lauren Silvis, The Wall Street Journal
Camus on Coronavirus
by Alain de Botton
Pandemics Kill Compassion, Too
by David Brooks
I Spent a Year In Space, and I have Isolation Tips to Share
by Scott Kelly, astronaut
For Those Struggling to Stay Sober, Coronavirus Shutdowns Offer Hope as Well as Temptation
by Sarah Hepola, for CNN (March 25, 2020)
The Coronavirus Inflicts Its Own Kind of Terror
People have always responded to epidemics by spreading rumor and false information, and portraying the disease as foreign and brought in with malicious intent.
By Orhan Pamuk, in The New York Times | Opinion
Mr. Pamuk was awarded the Nobel Prize in Literature in 2006.
April 23, 2020
ISTANBUL — For the past four years I have been writing a historical novel set in 1901 during what is known as the third plague pandemic, an outbreak of bubonic plague that killed millions of people in Asia but not very many in Europe. Over the last two months, friends and family, editors and journalists who know the subject of that novel, “Nights of Plague,” have been asking me a barrage of questions about pandemics.
They are most curious about similarities between the current coronavirus pandemic and the historical outbreaks of plague and cholera. There is an overabundance of similarities. Throughout human and literary history what makes pandemics alike is not mere commonality of germs and viruses but that our initial responses were always the same.
The initial response to the outbreak of a pandemic has always been denial. National and local governments have always been late to respond and have distorted facts and manipulated figures to deny the existence of the outbreak.
In the early pages of “A Journal of the Plague Year,” the single most illuminating work of literature ever written on contagion and human behavior, Daniel Defoe reports that in 1664, local authorities in some neighborhoods of London tried to make the number of plague deaths appear lower than it was by registering other, invented diseases as the recorded cause of death.
Not Like the Flu, Not Like Car Crashes, Not Like...
It's about the spike.
By Ari Schulman, Brendan Foht, Samuel Matlack, The New Atlantis
Published April 17, 2020 Updated April 18, 2020
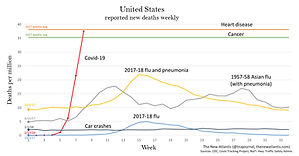
How deadly is Covid-19 compared to seasonal flu, past pandemics, or car crashes?
To offer context, we have produced two charts showing coronavirus deaths along with deaths from other common causes in the past to which the disease has recently been compared. One chart shows deaths for the United States, the other for New York, the state hardest hit.
Note that the data sets begin at different points in the year (as marked on the left). Also note that the figures shown here are for new deaths each week, not for cumulative deaths.
United States
The chart shows deaths per capita to allow for comparison of data from different years. Deaths are shown from:
-
Covid-19, starting from February 17. (Covid Tracking Project)
-
The 2017-18 flu season: This was the deadliest recent flu season. The chart shows one line for deaths attributed directly to flu, and another for deaths attributed to either flu or pneumonia. The smaller line is an undercount of flu-caused deaths, the larger is an overcount, with the real number lying somewhere in between. (More on this below.) The data begin on October 1, 2017, which the CDC considered the first week of that flu season. (CDC)
-
Heart disease and cancer: The first and second leading causes of death in the United States. The chart shows total 2017 deaths averaged per week. (CDC)
-
Car crashes: Weekly deaths beginning from January 1, 2018. (National Highway Traffic Safety Administration)
-
1957-58 Asian flu pandemic: Weekly influenza and pneumonia deaths beginning from August 24, 1957. These data come from a contemporary CDC program that surveilled 108 American cities with a total population of about 50 million people. We have used that figure, rather than the total U.S. population at the time, to calculate deaths per million. (CDC)
Let's Get Real About Coronavirus Tests
There aren’t enough. Many are shoddy. Most aren’t even designed to tell us what we really want to know.
By Michael T. Osterholm and Mark Olshaker
Mr. Osterholm is an infectious disease expert. Mark Olshaker is a writer and documentary filmmaker.
April 28, 2020, 5:00 a.m. ET
In the world’s ongoing quest to respond to the SARS-CoV-2 coronavirus, one of the tools most often invoked and hailed is testing — testing for current infections, to determine who is ill and contagious, and testing for antibodies, a sign of past infection and possibly, too, of future immunity.
The goal is to identify people who might spread the virus and isolate them, and to allow anyone protected from reinfection to resume an active social and professional life.
Democrats in the United States Senate have proposed a plan for “fast, free testing in every community.” At a recent news briefing, Andrew M. Cuomo, the governor of New York State, declared: “The more testing, the more open the economy.” President Trump’s new business advisory council has warned that the American economy will not rebound until wide-scale screening takes place.
But there are major problems with this approach. Far too few tests are available in the United States. Some are shoddy. Even the ones that are precise aren’t designed to produce the kind of definitive yes-no results that people expect.
The first type of test, the reverse transcription polymerase chain reaction (RT-PCR) test, diagnoses SARS-CoV-2 infections by analyzing cells collected from the nose or back of the throat. It converts the cells’ RNA into DNA and then, using polymerase enzymes, duplicates the DNA again and again, so that there’s enough of the virus that it can be detected, if it is present at all. This process is known as “amplification.”
As of April 27, about 5,593,000 such tests had been performed in the United States, according to the COVID Tracking Project. That’s far less testing, per capita, than in many other advanced countries, and it’s not nearly enough, especially since people will need to be screened repeatedly: Anyone who tests negative for SARS-CoV-2 today could be exposed to it tomorrow, particularly in areas where the virus is spreading rapidly.
Why Doesn't the Flu Tank Economy Like Covid-19?
Comparisons between two diseases—based on infections and deaths—missed range of differences
By Jo Craven McGinty, The Wall Street Journal
Updated April 10, 2020 5:53 p .m. ET
As one state after another issued economy-wrecking stay-at-home orders to counter the spread of the new coronavirus, skeptics asked a confounding question: Millions of Americans get the flu each year, and tens of thousands die from it. Why doesn’t the flu cause a shutdown?
According to the Centers for Disease Control and Prevention, up to 55 million Americans got the flu this season, and as many as 63,000 died. In comparison, more than 490,000 have been diagnosed with Covid-19, according to Johns Hopkins University, and more than 18,000 have died.
But the numbers don’t tell the whole story.
For starters, the flu tallies are estimates of total flu burden, while the Covid-19 figures are confirmed cases only. Eventually, the CDC will estimate the total Covid-19 burden, but for now, the numbers are not an apples-to-apples comparison.
“We always know confirmed cases are an underestimate,” said Lynnette Brammer, who leads the CDC’s domestic influenza-surveillance team.
In addition, Covid-19 differs from the flu in how quickly it spreads, the length and severity of the illness, and the unusual demands a contagion with no cure places on medical staff and facilities.
COVID-10: What's Wrong with the Models?
Originally written as an internal memo on April 15, 2020; updated and
shared publicly on April 20
April 20, 2020
The COVID-19 pandemic is constantly evolving, but where we stand today looks a lot different than where we stood a month ago. The good news is that it doesn’t look nearly as catastrophic as it seemed in mid-March. The numbers of new cases and new deaths seem to be plateauing and even declining (slightly) in hotspots such as New York City. So now we are at a fork in the road, as the diagram above suggests. Do we continue the “lockdowns” in hard-hit parts of the country, to halt the further spread of the disease? Or do we begin to open up parts of the population (and economy), and inch back towards something resembling “normal?”
To contemplate, let alone answer, this question really digs into a much deeper question about the current state of affairs and how we got here. Are we in the somewhat favorable state we are in today because of how well we’ve contained the virus, how well we’ve “flattened the curve?” Or are we in this state because the SARS-CoV-2 virus is less deadly than we initially thought?
If possible, let’s try to have this discussion with as little emotion as possible. Instead, we should think about it through the lens of what we know about logic, supposition, and probabilities.
Is the Virus on My Clothes? My Hair? My Shoes? My Newspaper?
We asked the experts to answer questions about all the places coronavirus lurks (or doesn’t). You’ll feel better after reading this.
By Tara Parker-Pope, The New York Times
Published April 17, 2020 Updated April 18, 2020
When we asked readers to send their questions about coronavirus, a common theme emerged: Many people are fearful about tracking the virus into their homes on their clothes, their shoes, the mail and even the newspaper.
We reached out to infectious disease experts, aerosol scientists and microbiologists to answer reader questions about the risks of coming into contact with the virus during essential trips outside and from deliveries. While we still need to take precautions, their answers were reassuring.
Should I change my clothes and shower when I come home from the grocery store?
For most of us who are practicing social distancing and making only occasional trips to the grocery store or pharmacy, experts agree that it’s not necessary to change clothes or take a shower when you return home. You should, however, always wash your hands. While it’s true that a sneeze or cough from an infected person can propel viral droplets and smaller particles through the air, most of them will drop to the ground.
Studies show that some small viral particles could float in the air for about half an hour, but they don’t swarm like gnats and are unlikely to collide with your clothes. “A droplet that is small enough to float in air for a while also is unlikely to deposit on clothing because of aerodynamics,” said Linsey Marr, an aerosol scientist at Virginia Tech. “The droplets are small enough that they’ll move in the air around your body and clothing.”
COVID-19: Melatonin as a potential adjuvant treatment
Author: Rui Zhang, Xuebin Wang, Leng Ni, Xiao Di, Baitao Ma, Shuai Niu, Changwei Liu, Russel J. Reiter
Publication: Life Sciences
Publisher: Elsevier
Date: Available online 23 March 2020
© 2020 Published by Elsevier Inc.
Abstract: This article summarizes the likely benefits of melatonin in the attenuation of COVID-19 based on its putative pathogenesis. The recent outbreak of COVID-19 has become a pandemic with tens of thousands of infected patients. Based on clinical features, pathology, the pathogenesis of acute respiratory disorder induced by either highly homogenous coronaviruses or other pathogens, the evidence suggests that excessive inflammation, oxidation, and an exaggerated immune response very likely contribute to COVID-19 pathology. This leads to a cytokine storm and subsequent progression to acute lung injury (ALI)/acute respiratory distress syndrome (ARDS) and often death. Melatonin, a well-known anti-inflammatory and anti-oxidative molecule, is protective against ALI/ARDS caused by viral and other pathogens. Melatonin is effective in critical care patients by reducing vessel permeability, anxiety, sedation use, and improving sleeping quality, which might also be beneficial for better clinical outcomes for COVID-19 patients. Notably, melatonin has a high safety profile. There is significant data showing that melatonin limits virus-related diseases and would also likely be beneficial in COVID-19 patients. Additional experiments and clinical studies are required to confirm this speculation.
Camus on Coronavirus
By Alain de Botton
Mr. de Botton is a writer and philosopher
In January 1941, Albert Camus began work on a story about a virus that spreads uncontrollably from animals to humans and ends up destroying half the population of “an ordinary town” called Oran, on the Algerian coast. “The Plague,” published in 1947, is frequently described as the greatest European novel of the postwar period.
As the book opens, an air of eerie normality reigns. The town’s inhabitants lead busy money-centered and denatured lives. Then, with the pacing of a thriller, the horror begins. The narrator, Dr. Rieux, comes across a dead rat. Then another and another. Soon an epidemic seizes Oran, the disease transmitting itself from citizen to citizen, spreading panic in every street.
I Spent a Year in Space, and I Have Isolation Tips to Share
By Scott Kelly, astronaut
Being stuck at home can be challenging. When I lived on the International Space Station for nearly a year, it wasn’t easy. When I went to sleep, I was at work. When I woke up, I was still at work. Flying in space is probably the only job you absolutely cannot quit.
But I learned some things during my time up there that I’d like to share — because they are about to come in handy again, as we all confine ourselves at home to help stop the spread of the coronavirus. Here are a few tips on living in isolation, from someone who has been there.
Ten Weeks to Crush the Curve
By Harvey V. Fineberg, in The New England Journal of Medicine | Editorial
April 1, 2020
The President says we are at war with the coronavirus. It’s a war we should fight to win.
The economy is in the tank, and anywhere from thousands to more than a million American lives are in jeopardy. Most analyses of options and trade-offs assume that both the pandemic and the economic setback must play out over a period of many months for the pandemic and even longer for economic recovery. However, as the economists would say, there is a dominant option, one that simultaneously limits fatalities and gets the economy cranking again in a sustainable way.
That choice begins with a forceful, focused campaign to eradicate Covid-19 in the United States. The aim is not to flatten the curve; the goal is to crush the curve. China did this in Wuhan. We can do it across this country in 10 weeks.
And with enough intelligence about the enemy — where the virus lurks, how quickly it is moving, where it is most threatening, and what its vulnerabilities are — we can begin to re-energize the economy without putting additional lives at risk.
If we take these six steps to mobilize and organize the nation, we can defeat Covid-19 by early June.
The Road Back to Normal: More, Better Testing
Rapid diagnosis, targeted surveillance and boosting lab supplies will help beat back the coronavirus
The Wall Street Journal OPINION | COMMENTARY
By Scott Gottlieb and Lauren Silvis
March 29, 2020 135 pm ET
Americans are afraid of the health risks from Covid-19. But many also rightfully worry about when the intense restrictions on movement and activity will end. Addressing both concerns will require setting up a robust testing system that can catch outbreaks before they become difficult to manage.
April will be a hard month as the epidemic spreads across the nation. The priorities are maintaining the health-care system, preserving life, protecting the vulnerable, and supporting the economy. The epidemic may calm down by July and August, but Covid-19 is likely to be seasonal and could return with a vengeance in the fall.
How do we crack the current outbreak, develop a plan to return to normal life, and ensure that the virus never poses the same threat again? That will require a system that can detect when the virus is spreading. The system would have three components: is spreading. The system would have three components:
Pandemics Kill Compassion, Too
By David Brooks
Some disasters, like hurricanes and earthquakes, can bring people together, but if history is any judge, pandemics generally drive them apart. These are crises in which social distancing is a virtue. Dread overwhelms the normal bonds of human affection.
In “The Decameron,” Giovanni Boccaccio writes about what happened during the plague that hit Florence in 1348: “Tedious were it to recount how citizen avoided citizen, how among neighbors was scarce found any that shewed fellow-feeling for another, how kinfolk held aloof, and never met … nay, what is more, and scarcely to be believed, fathers and mothers were found to abandon their own children, untended, unvisited, to their fate.”
For Those Struggling to Stay Sober, Coronavirus Shutdowns Offer Hope as Well as Temptation
by Sarah Hepola, for CNN (March 25, 2020)
There's no easy time to get sober, but a global pandemic is tougher than most.
Back when I was trying and failing to quit, I'd reach for any excuse to bail on my better self. A bad day. A text from my ex, or no text.
One day, a snowstorm walloped the city, shuttering my office, and I pulled on my rubber boots with a sigh as if to say, "I guess I'm drinking now."
I didn't want to be this person, passing out on the futon with the television flickering on her face, waking up to green empties mashed with cigarette butts, but I didn't know another way.